Aged care compliance
SIRS for Support at Home Providers: The New Compliance Reality Under the Aged Care Act 2024
Until recently, SIRS reporting only applied inside the four walls of a residential aged care facility. From 1 November 2025, it follows your staff out the door and into every home they visit.
For five years, the Serious Incident Response Scheme (SIRS) was a residential aged care problem. If you ran a home care package, you had your own lighter-touch incident notification regime, and that was that. That changed on 1 November 2025. From that date, every registered provider delivering Support at Home services — personal care, nursing, clinical care, allied health, domestic assistance with care components — carries the same SIRS reporting obligations as a 120-bed residential facility. The categories, the timeframes, the investigation requirements, and the civil penalties (up to $1.58 million for body corporates — 4,800 penalty units at the current penalty-unit value under section 48AB of the Aged Care Act 2024) all apply.
For a sector that has historically thought of compliance in terms of client files and care plans, this is a step-change. Home care is now regulated under a scheme designed for institutions. The providers who handle this transition well will redesign their incident workflow, train every frontline worker on the eight reportable categories, and give their clinical leads a way to escalate and report incidents within hours, not weeks. The providers who treat it as a paperwork exercise will find themselves in front of the Aged Care Quality and Safety Commission (ACQSC) explaining why a Priority 1 incident sat in someone's inbox for 36 hours.
This guide walks through what changed, who is in scope, and what a compliant SIRS workflow looks like for a Support at Home provider in 2026.
What actually changed on 1 November 2025
The Aged Care Act 2024 commenced on 1 November 2025, replacing the Aged Care Act 1997. Two things happened at the same time:
- The Home Care Packages program was retired and replaced by the new Support at Home program.
- The SIRS framework, which had previously applied to residential care only, was extended to all registered providers delivering personal care, nursing, clinical care, or allied health services in a home or community setting.
In practical terms, this means a personal care worker visiting a consumer at 7am on a Tuesday morning can now trigger a SIRS notification if the incident they observe meets one of the eight reportable categories. The obligation lands on the registered provider, not on the individual worker. The "becoming aware" clock starts when a senior staff member — typically the care manager, clinical lead, or nominated person — receives the report, not when the incident occurs.
The categories and the deadlines did not change. They are identical to the residential regime that has been in place since April 2021. What changed is the population of providers now subject to them.
Who is in scope
The simplest way to think about it: if your service is personal care, clinical care, nursing, or allied health delivered to a consumer in their home or in a community setting, and you are a registered provider under the new Act, you are in scope. This includes:
- Providers delivering personal care services (bathing, dressing, grooming, toileting, mobility assistance)
- Providers delivering clinical nursing care in the home (wound care, catheter care, medication administration)
- Providers delivering allied health services in the home (physiotherapy, occupational therapy, dietetics, podiatry)
- Providers delivering domestic assistance where the service is part of a broader care package
- Providers delivering respite care in the home
The ACQSC has been clear that the obligation is on the provider, not on the individual worker. But the worker is the trigger — they are the eyes and ears in the home. That has practical implications for how you design your incident escalation workflow, which we will cover below.
The 8 reportable incident categories
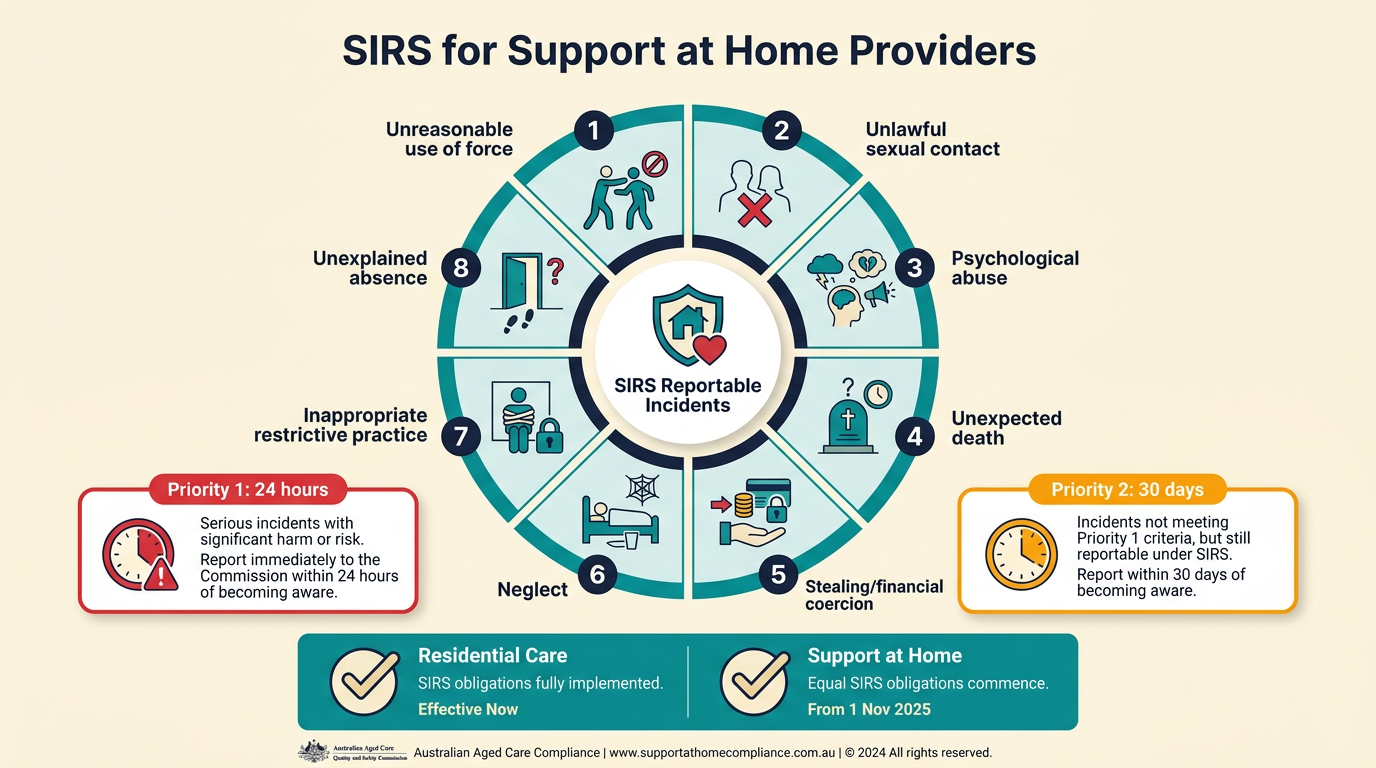
The categories are unchanged from the residential regime. They are intentionally broad — the Commission expects providers to report early and investigate thoroughly, rather than wait for certainty. The eight categories are:
- Unreasonable use of force — physical contact that is disproportionate, unnecessary, or not in the consumer's best interest. Includes rough handling during personal care, inappropriate physical interventions, and any use of force beyond what is clinically justified.
- Unlawful sexual contact — any sexual contact without consent, or where consent cannot be given due to cognitive impairment. This is always classified as Priority 1.
- Psychological or emotional abuse — verbal abuse, threats, intimidation, humiliation, or patterns of behaviour that cause psychological harm. Includes yelling at consumers, derogatory comments, and deliberate social isolation.
- Unexpected death — a death that is not consistent with the consumer's known clinical condition or care plan. This includes deaths during or shortly after a fall, medication error, choking incident, or unexplained circumstances.
- Theft or financial coercion — theft of property or money, coercion to change wills or financial arrangements, or misuse of powers of attorney.
- Neglect — failure to provide adequate care, supervision, or services. Includes missed medications, failure to respond to clinical deterioration, inadequate nutrition or hydration, and failure to implement care plans.
- Inappropriate use of restrictive practices — any use of physical, chemical, mechanical, or environmental restraint, or seclusion, that is not authorised under a behaviour support plan, not used as a last resort, or used without informed consent.
- Unexplained absence from care — a consumer who is missing from the service and whose absence is unexplained and unusual given their care needs and cognitive status.
The obligation to report is triggered when the provider becomes aware that an incident falls within one of these eight categories — regardless of whether serious harm actually resulted. This is an important distinction that catches many providers off guard during ACQSC assessment contacts.
Priority 1 vs Priority 2: the deadlines
SIRS incidents are classified by priority, which determines the reporting timeframe. The timeframes are tight:
- Priority 1 — incidents that caused, or could reasonably have caused, significant harm to a consumer. Must be reported to the Commission within 24 hours of the provider becoming aware of the incident.
- Priority 2 — incidents that caused, or could reasonably have caused, harm that was not significant. Must be reported within 30 days of becoming aware.
For a Support at Home provider, the "becoming aware" moment is typically when the personal care worker or clinician returns to the office, completes their visit notes, and flags the incident to a senior staff member. Some providers are configuring their mobile worker apps to require a structured incident note before the visit can be closed — that timestamp then becomes the start of the 24-hour or 30-day clock.
What the Commission expects after a notification
A SIRS notification is not a one-off report. It is the start of a structured investigation cycle. For every Priority 1 or Priority 2 notification, the Commission expects the following:
- Initial notification — submitted via the My Aged Care portal, including the incident category, priority level, brief description, and immediate actions taken
- Full investigation report — within the timeframe the Commission sets in its response to the notification (common defaults are 60 days for Priority 1 and 90 days for Priority 2); the Commission's letter always overrides these defaults
- Witness statements — from the staff involved, the consumer (where appropriate), and family members
- Linked evidence — visit notes, clinical notes, medication charts, photographic evidence where relevant, and any other supporting documents
- Corrective actions — what the provider has done, is doing, and will do to prevent recurrence, with owners and due dates
- Closure evidence — evidence that the corrective actions have been completed and the underlying issue is resolved
For a Support at Home provider, the "linked evidence" step is the one that most often falls down. Workers in the field capture visit notes on mobile apps, but the evidence trail is often fragmented — a note here, a photo there, a verbal handover there. Assembling a complete evidence pack in the 60- or 90-day investigation window requires that everything be linked to a single incident record from the moment the notification is created.
Common SIRS mistakes specific to home care
The Commission has been publishing provider non-compliance findings since 2021. From those findings, the most common mistakes specific to Support at Home providers are:
- Late reporting from the field. A personal care worker observes a Priority 1 incident but waits until their next office day to report it. The 24-hour window is already half gone before anyone in a senior role becomes aware.
- Unclear incident ownership. The incident is reported to a coordinator who is on annual leave. The "becoming aware" clock is ambiguous, and the provider cannot demonstrate compliance with the deadline.
- Misclassification as a "client complaint." A family member reports an incident that meets the definition of psychological or emotional abuse. The provider logs it as a complaint and investigates internally, missing the obligation to notify the Commission.
- Incomplete visit-note linkage. The investigation requires the worker's visit notes from the day of the incident. The notes are in a separate system, not linked to the SIRS record, and the provider cannot produce them within the Commission's timeframe.
- No family communication step. Under the strengthened Quality Standards, families must be informed of serious incidents affecting their loved one. Missing this triggers a separate Quality Standard non-compliance on top of the SIRS failure.
- No quarterly aggregate review. SIRS is not just about individual incidents. The Commission expects providers to spot patterns across notifications and act on them. A quarterly aggregate review is the standard the Commission looks for.
What a compliant Support at Home SIRS workflow looks like
The Support at Home providers who handle SIRS well have redesigned their incident workflow around the 24-hour and 30-day clocks. The key elements are:
- Mobile-first incident reporting. Every frontline worker can file an incident report from their phone, in under two minutes, with structured fields for category, priority, and immediate actions. The timestamp is captured at the moment of submission, not at the end of the day.
- Automatic escalation. When a Priority 1 incident is filed, the system immediately notifies the care manager, clinical lead, and a backup contact. If none of them acknowledge within 30 minutes, the alert escalates to the CEO or nominated person.
- Deadline tracking with alerts. The 24-hour and 30-day deadlines are calculated and tracked. Alerts fire at 12 hours, 6 hours, and 1 hour remaining for Priority 1, and at 21 days, 25 days, and 28 days for Priority 2.
- Linked evidence from the start. Visit notes, photos, witness statements, and corrective actions are all linked to the incident record from the moment they are created. The investigation report pulls from a single source of truth.
- Family communication as a workflow step. The family is informed within hours of the incident (not days), kept updated during the investigation, and briefed on the outcome. This is a required step, not an optional one.
- Quarterly aggregate analysis. Patterns are surfaced automatically: the same type of incident in the same region, the same time of day, the same staff member, the same care plan gap. Patterns drive systemic change.
How NovoCove supports Support at Home SIRS
NovoCove is built around the SIRS workflow, and it works the same way whether your service is residential or home-based. When a worker reports an incident in the platform, the system:
- Prompts the right classification based on the incident type, with built-in decision support drawn from the ACQSC's own guidance
- Calculates the deadline based on priority (24 hours for Priority 1, 30 days for Priority 2) and starts the clock the moment a senior staff member is notified
- Sends escalating alerts as the deadline approaches, with built-in escalation to a backup contact if the primary contact is unavailable
- Links every piece of evidence — visit notes, photos, witness statements, corrective actions — to the incident record from the moment it is created
- Tracks the investigation log with timestamped entries and produces the Commission investigation report in the format the regulator expects
- Captures corrective actions with owners and due dates, and tracks them to closure with evidence
- Generates the quarterly SIRS aggregate report for the Commission automatically, with the patterns surfaced for your clinical governance review
- Maintains the full audit trail (minimum 7 years on the Professional plan and above), with role-based access for the Commission during an assessment contact
For Support at Home providers, the critical difference is the mobile-first design. Workers in the field file incident reports from their phone, and the evidence captured at the point of care is linked to the SIRS record automatically. By the time the care manager opens the incident in the office, the 24-hour clock is already running and the escalation chain is already in motion.
The result is SIRS notifications that are accurate, on-time, and complete — whether your service operates inside a facility or in someone's living room.
This guide is general information and is not legal advice.