Aged care compliance
Care Minutes Supplement 2026: What Every Residential Aged Care Provider Must Prove to Keep Its Funding
From 1 April 2026, residential aged care funding in metropolitan Australia is no longer paid on roster promises — it is paid on proven delivery of 215 care minutes per resident per day, including 44 RN minutes. The Department of Health and Aged Care is introducing a new Care Minutes Supplement and a sliding-scale reduction of up to $31.64 per resident per day that hits the Base Care Tariff of any home that misses the target. Here is what the new mechanism means for your service, who is in scope, what the Commission will audit, and the quarterly reporting workflow that keeps the funding intact.
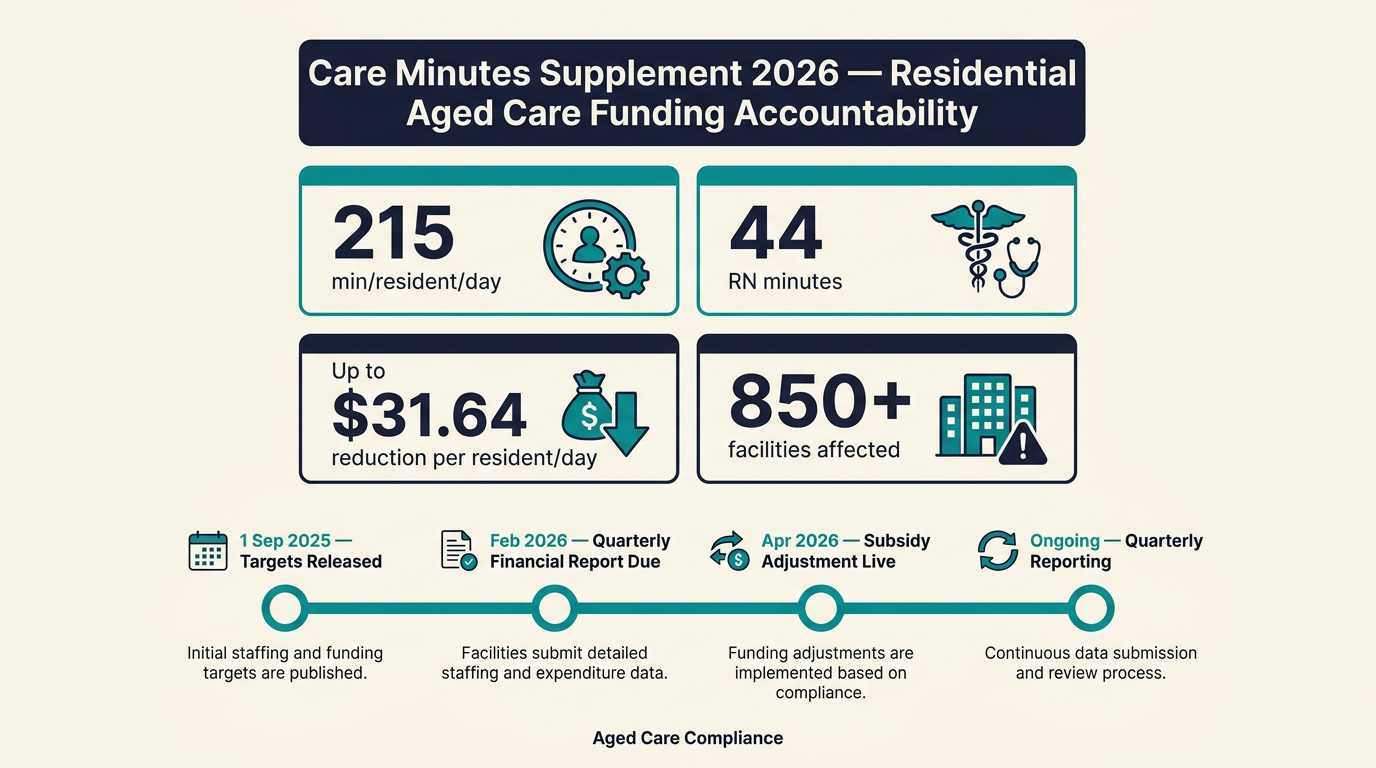
From 1 April 2026, residential aged care funding in metropolitan Australia is no longer paid on roster promises. It is paid on proven delivery of 215 care minutes per resident per day, of which at least 44 minutes must be delivered by a Registered Nurse on site. The Department of Health and Aged Care is rolling out a new Care Minutes Supplement and a sliding-scale reduction of up to $31.64 per resident per day that hits the Base Care Tariff of any home that misses the target. Sector analysts at Mirus Australia estimate that more than 850 MM1 metropolitan facilities will be in scope of the first wave of funding adjustments, and the consequences of getting it wrong compound every quarter.
This is the biggest funding-side compliance change in residential aged care since the AN-ACC funding model replaced the Aged Care Funding Instrument in 2022. It moves care minutes from a "best efforts" target to a line item on your Quarterly Financial Report, and from an internal quality metric to a dollar figure on the Commonwealth subsidy. For every residential provider in a Modified Monash 1 area, the question is no longer "do we think we are meeting the target?" — it is "can we prove it, with timestamps and roster data, to a funder who will read it differently from a regulator who will audit it differently?"
What are care minutes, and where do the 215 and 44 come from?
Care minutes are a count of the direct, hands-on time that nurses and carers spend with residents. The Department of Health and Aged Care defines the count by activity type, not by shift length: clinical care (medications, wound care, assessments), personal care (showering, dressing, toileting, meals), mobility support, and social and emotional support — particularly for residents living with dementia. A small amount of care planning and family liaison time can also count.
The 215 and 44 numbers are national average targets. They were set out in the 2022-23 Budget measures that accompanied the new AN-ACC funding model, then progressively raised each year. The 2026 figure of 215 total minutes (44 RN) is the headline target that applies to all mainstream residential care, and the 24/7 onsite Registered Nurse rule layers on top — a separate, parallel obligation that runs from 1 July 2023 in metropolitan and regional homes and from 1 October 2024 in rural and remote homes.
- 215 total direct care minutes per resident per day — averaged across the home, calculated from roster and payroll data, and reported quarterly.
- 44 Registered Nurse minutes per resident per day — the RN-only slice of the 215, also averaged across the home.
- 24/7 onsite RN — a separate obligation that an RN must be physically present in the home at all times, not on call and not covering multiple sites.
- Mandatory care minute reporting — homes submit actual minutes delivered via the Quarterly Financial Report (QFR) to Services Australia.
These are the same targets that have applied since 1 October 2024, but the difference from 1 April 2026 is what happens when you miss them. Until April 2026, the targets were a published expectation with quarterly visibility but no automatic funding consequence. From April 2026, missing the target reduces your Base Care Tariff automatically, every quarter, on a published sliding scale.
What changes from 1 April 2026: the funding mechanism
The mechanism has three parts: a sliding-scale reduction to the Base Care Tariff, a new Care Minutes Supplement payment, and a published calculation that ties both to a single three-month reporting period. The Department of Health and Aged Care published the framework in the Care Minutes funding changes fact sheet, and the 30 September 2025 Office of Impact Analysis paper sets out the policy rationale and the modelled sector impact.
The Base Care Tariff reduction is the consequence side. From 1 April 2026, every MM1 residential aged care home that does not meet the 215 total care minutes target — or the 44 RN minutes target — will see a per-resident-per-day reduction in the Base Care Tariff it is paid. The maximum reduction is $31.64 per resident per day, applied on a sliding scale: the further you are from the target, the larger the reduction. Both the total minutes target and the RN minutes target are tested separately, and a failure on either axis can trigger a reduction.
The Care Minutes Supplement is the incentive side. Homes that meet both the 215 and 44 targets in a given quarter receive an additional per-resident-per-day supplement on top of the Base Care Tariff. The supplement is designed to roughly offset the operational cost of delivering the additional minutes, and it is paid in the same quarterly cycle as the Base Care Tariff. A home that meets the targets for three consecutive quarters also builds a compliance buffer: a one-quarter miss in the following year will not trigger a Base Care Tariff reduction if the rolling average holds.
Who is in scope: MM1, MM2 and the metropolitan / non-metropolitan split
The 1 April 2026 funding accountability applies in the first instance to MM1 (Modified Monash 1) facilities — that is, metropolitan residential aged care homes in the major capital cities and their inner surrounds. MM2 to MM7 homes (regional, rural and remote) are out of scope for the first wave, and the existing voluntary quarterly reporting continues to apply to those homes.
The Modified Monash Model is the same classification used for the rural loading on the Medicare Benefits Schedule, the Distribution Priority Area for GP workforce, and the rural loading in the National Disability Insurance Scheme. For aged care funding accountability, an MM1 designation is determined by the ABS remoteness area and the home's geographic location, not by the home's own classification of itself as "metropolitan".
- MM1 — capital cities and major metropolitan areas: the first wave of funding accountability from 1 April 2026.
- MM2 to MM7 — regional, rural and remote areas: voluntary quarterly reporting, no Base Care Tariff reduction for missing the target, but the published targets still apply.
- Specialised homeless, Aboriginal and Torres Strait Islander, and short-term restorative care homes — different funding arrangements; consult the Department fact sheet for the applicable care minute equivalent.
If your service is in an MM1 area, the 1 April 2026 date is firm. If your service is in MM2 to MM7, the 1 April 2026 Base Care Tariff reduction does not apply, but the care minute targets and the 24/7 RN rule still do, and the published quarterly reporting is a leading indicator of when the funding accountability will extend to your classification.
Reporting: the Quarterly Financial Report, the calculation period, and the deadline
The funding adjustment is driven by the care minutes you delivered in a prior three-month period. The Department calls this the calculation period, and it is the first mechanism by which care minute reporting becomes a financial artefact rather than a clinical artefact. The first calculation period was 1 June to 31 August 2025, and the first adjusted subsidy was paid in the April 2026 quarter. After that, every quarter's subsidy is adjusted based on the prior quarter's delivery.
The data the Department uses is the roster and payroll data that the home submits via the Quarterly Financial Report (QFR) on the Services Australia portal. The QFR was already a published reporting requirement; the 1 April 2026 change is that the care minute fields on the QFR are now read as the input to a funding formula, not just a compliance statistic. The targets themselves are also published on 1 September each year, so the home knows in advance what the next calculation period will be tested against.
- 1 September 2025 — Department of Health and Aged Care published the 2026 care minute targets (215 total, 44 RN) and the per-resident-per-day Base Care Tariff reduction schedule.
- June to August 2025 — first calculation period. The QFR for this period was the first input to the funding formula.
- February 2026 — QFR submission deadline for the June to August 2025 calculation period. The submitted data is locked in as the basis for the April 2026 subsidy.
- 1 April 2026 — first adjusted subsidy implemented. The Base Care Tariff paid from this date reflects the calculation period results.
- Ongoing — every quarter thereafter, with a one-quarter lag between the calculation period and the subsidy adjustment.
The one-quarter lag is important operationally. By the time your home's Base Care Tariff is reduced in a given quarter, the calculation period that drove the reduction has already closed three months earlier. There is no re-submission, no appeal, and no late evidence. If your QFR for the June to August 2025 period showed a miss, the funding reduction lands in April 2026 and is paid every day from then on until a subsequent calculation period shows you are back on target.
The 5-step workflow that protects the funding
The mechanism is unforgiving, but the workflow to stay on the right side of it is straightforward. It is a quarterly cycle that runs in parallel to your existing roster and payroll cycle, with one new artefact: a published care minute dashboard that the leadership team and the funding manager both read every week.
- Map the calculation period in advance. Pull the published targets on 1 September, then identify the three months that will be the next calculation period. Lock those dates into the funding team's calendar and the roster team's planning cycle. The calculation period is the only window that matters — everything else is lead time.
- Forecast care minutes weekly, not monthly. Use roster data, AN-ACC classifications and known resident admissions or discharges to forecast the rolling weekly average of total minutes and RN minutes. Flag any week that is tracking below 215 or below 44 before the week closes, not after.
- Treat the 24/7 RN rule as a hard constraint, not a stretch goal. A home that meets the 215 total minutes target but does not have an RN physically on site at all times will fail the parallel 24/7 RN obligation. The two are tested separately and both feed the QFR. Roster the RNs first, then backfill the rest of the team.
- Reconcile the QFR data before submission. The QFR pulls roster and payroll data automatically, but the care minute classification of each shift (clinical, personal, mobility, social) is mapped from the roster codes. Audit the mapping quarterly — a small misclassification across a single shift type can move the rolling average below 44 RN minutes for the calculation period.
- Hold a quarterly funding-and-rostering review. The funding team and the rostering team need to look at the same data, in the same room, on the same day, every quarter. The output is a one-page summary: did we meet the target, what is the projected Base Care Tariff for next quarter, and what roster changes are needed to hold the target for the next calculation period.
What the ACQSC will look at during an audit
The Aged Care Quality and Safety Commission is the regulator that audits compliance with the strengthened Quality Standards that took effect on 1 November 2025 under the new Aged Care Act 2024. The new audit process — which rolled out across categories 4, 5 and 6 from 29 April 2026 — has its own focus, but the care minute funding data is now a parallel evidence stream that the Commission can and does request during a site audit.
What the Commission is looking for is whether the care minutes the home reports to the funder match the care minutes the residents actually receive. That means three layers of evidence: the roster and payroll data submitted on the QFR, the shift-level records the home keeps internally, and the resident care plans and progress notes that show who received what care and when. If the three layers don't line up, the home has a documentation problem that the Commission will treat as a governance failure under Standard 1 (the organisational governance standard) and Standard 4 (the care delivery standard).
- Standard 1 — Organisational governance — the governing body must be able to demonstrate oversight of the care minute obligations, not just the care delivery team.
- Standard 4 — Care delivery — the actual care minutes must align with the assessed needs of the residents in the home, not just the published target.
- Standard 6 — Feedback and complaints — residents and families must have a documented channel to raise concerns about staffing levels, and the home must be able to show how those concerns were investigated and resolved.
How NovoCove handles this
NovoCove was built for Australian residential aged care providers who need to prove compliance on demand, not just at the next audit visit. The platform gives your funding team and your rostering team a single source of truth for the 215 and 44 targets: live care minute dashboards that pull from your existing payroll and rostering system, weekly forecast reports that flag any calculation period that is tracking below target, and a QFR-ready evidence pack that the funding manager can attach to the quarterly submission without a manual reconciliation.
On the governance side, NovoCove gives the board and the CEO a single-page view of the funding accountability obligations under the new Aged Care Act — the 24/7 RN rule, the QFR deadlines, the published calculation periods, and the rolling average of care minute delivery across the home. Every audit trail is timestamped, every roster change is logged, and every gap between the published target and the actual delivery is visible to the leadership team before it becomes a funding reduction.
Whether you are an MM1 home in the first wave of funding accountability or an MM2 to MM7 home that will be in the second wave, the workflow is the same. Book a 20-minute walkthrough and we will show you what your home would look like under the new funding model, with your real roster data, before the next calculation period closes.
This guide is general information and is not legal advice.